During my research I came across multiple TED Talks, that sounded really interesting to my topic of first aid for epilepsy. I decided to run a TED Talk watching session to learn about the most recent extraordinary findings and discussions about brain-sensing technologies. I did this, because the concept of my existing prototype relies on seizure detection to start an app alert to nearby bystanders to provide first aid. I had a look on the following with TED Talks:
Forecasting and preventing epileptic seizures
David Garrett’s 2022 TED Talk, Listening to the Brain: A Functional Cure for Epilepsy, dives into how neuromodulation implants can provide a „functional cure“ for epilepsy. His research shows that it is possible to predict seizures by tracking electrical activity in the brain. Garrett explains how brain excitability levels that exceed a certain threshold lead to an electrical storm, triggering seizures. His team developed ultra-thin carbon fiber electrodes to be placed into brains of living humans. This sensor technology is integrated into an epilepsy management system. These electrodes wirelessly transmit data, allowing AI-powered algorithms to detect seizure patterns and intervene before a seizure occurs.
Garrett’s work makes an example of the immense potential of brain-sensing technology. Once it is accessible for consumers, such advancements could drastically improve the quality of life for epilepsy patients. The ability to predict and prevent seizures could make constant supervision or emergency first aid not needed anymore. However, continuous brain monitoring raises concerns about user acceptance – how comfortable would individuals be, if they know their brain activity is being monitored and potentially controlled? While the technology offers freedom from seizures, it may also introduce anxieties about privacy and autonomy.
AI wearables for seizure detection
Rosalind Picard’s 2018 talk, An AI Smartwatch That Detects Seizures, builds upon this concept by demonstrating how AI-powered wearables can recognize seizures and alert caregivers. Her work was inspired by cases of Sudden Unexpected Death in Epilepsy (SUDEP), which claims lives more frequently than sudden infant death syndrome. The smartwatch, developed by her company Empatica, runs real-time AI to detect generalized tonic-clonic seizures and has received FDA approval. This could be a game-changer for people with epilepsy, enabling immediate emergency response and reducing deaths. However, as with Garrett’s implantable devices, widespread adoption will depend on user trust and data privacy assurances. Real-time health data collection is extremely valuable for medical purposes, but it also opens the door for potential misuse.
Breaking the stigma around epilepsy
Besides technological advancements, societal perceptions of epilepsy significantly impact those affected. Sitawa Wafula’s 2017 TED Talk, Why I Speak Up About Living with Epilepsy, highlights the emotional and psychological struggles individuals face. She describes losing her job and dropping out of school due to her seizures, leading to isolation and frustration. Through online blogging and advocacy, she found a way to empower others and change the narrative around epilepsy. Wafula’s talk shows the importance of combining technological advancements with public awareness and support systems. Brain-sensing technologies can provide medical solutions, but addressing stigma and ensuring societal acceptance are equally crucial for improving patients’ lives.
Ethical dilemmas in brain data privacy
Nita Farahany’s 2023 TED Talk, Your Right to Mental Privacy in the Age of Brain-Sensing Tech, shifts the conversation towards the ethical aspects of neurotechnology. As major tech companies integrate brain sensors into everyday devices – such as headbands, earbuds and watches – brain activity is becoming increasingly transparent. Farahany warns that while brain-sensing technology has immense potential for treating conditions like epilepsy and PTSD, it also presents unprecedented privacy risks.
Brain data is more sensitive than any other form of personal data. It can reveal emotions, preferences and thoughts, raising concerns about microtargeting and behavioral manipulation. Farahany calls for the recognition of cognitive liberty as a fundamental human right, which means that individuals must have control over their own brain data. Without well-thought ethical frameworks, neurotechnology could become a tool for surveillance and control rather than empowerment.
Expanding Our Understanding of the Brain
Finally, Ed Boyden’s 2016 TED Talk, A New Way to Study the Brain’s Invisible Secrets, presents an approach to understanding the brain’s microscopically small structures. Boyden’s team developed a technique using expandable materials – similar to those found in baby diapers – to enlarge brain tissue for easier examination. By physically expanding the brain, researchers can distinguish between biomolecules and recognize structures that may be responsible for neurological diseases.
Boyden’s work emphasizes the importance of fundamental research in brain science. While neurotechnologies are advancing rapidly, they still rely on a limited understanding of brain function. By developing new ways to study the brain, scientists can create more effective examinations and medical professionals targeted treatments based on solid understanding rather than guesswork.
Conclusion
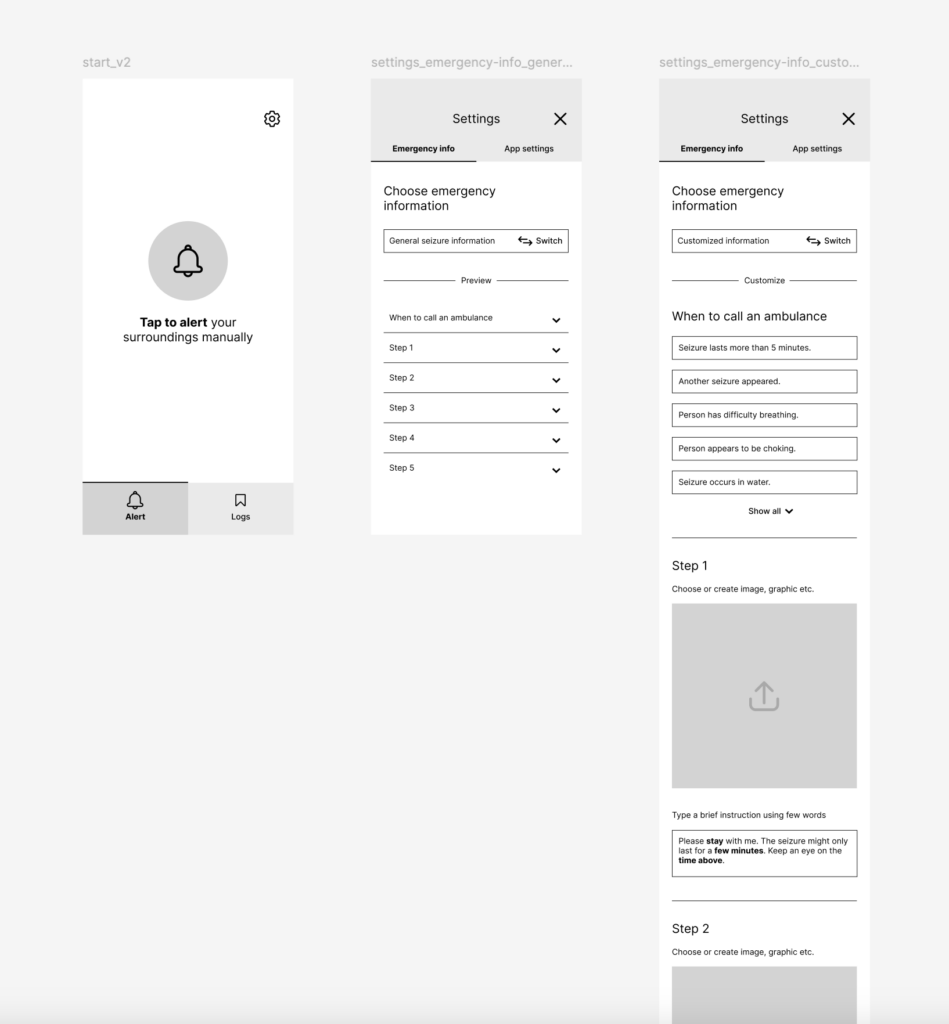
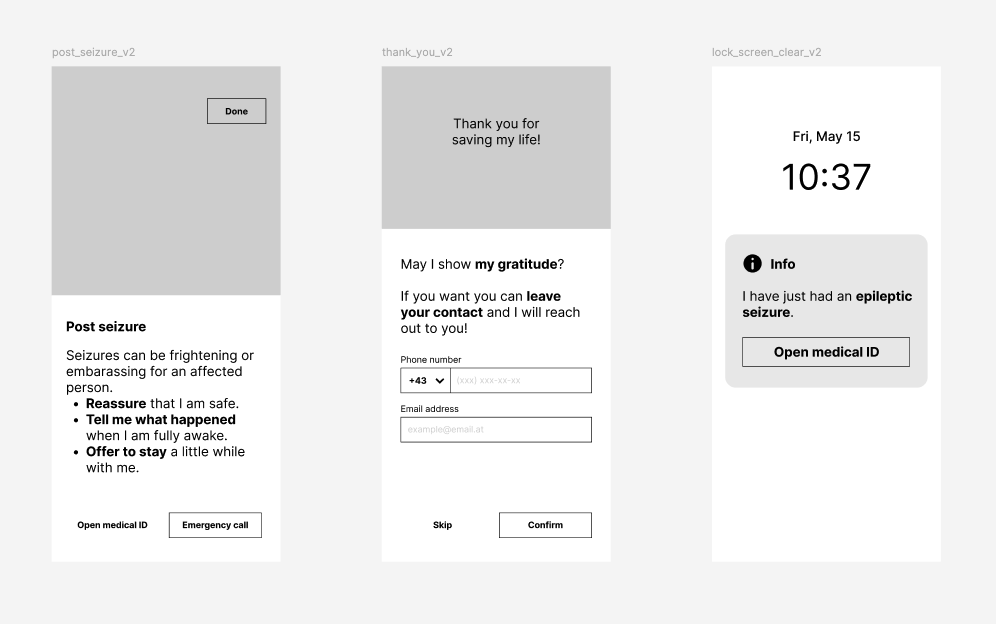
The concept for a first aid app for epilepsy I initially brought into a prototype, that is suppose to be powered by brain-sensing technology, could be of great importances in ensuring timely first aid by strangers and medical assistance. However, by integrating predictive algorithms and real-time AI monitoring, such an app would need to be shifted towards the scenario before a seizure occurs. Also if a unit is included, that prevents the brain to have electrical anomalies which would lead to non-occurring seizures, the usefulness of this app to provide first aid instruction to public bystanders significantly decreases.
However, the success of such a technology depends on trust and ethical considerations. Continuous brain monitoring comes with concerns about privacy, data security and user acceptance. If individuals are afraid how their brain data might be used or shared, they may not to use the technology. Regulatory measures and transparent policies must be in place to ensure that brain data remains protected and is only used for the benefit of the user.
Ultimately, while a first aid app for epilepsy has the potential to better first aid care, it must be developed with both innovation and ethical responsibility in mind. By addressing privacy concerns and prioritizing user autonomy, we can create a future where technology truly empowers those living with epilepsy.