With regards to the example of Aura: Seizure First Aid mentioned in the last blog post, I iterated on a paper prototype regarding „Ad Hoc First Aid Collaboration with the Public“. This prototype had its origin in an exercise at the very beginning of the course Design & Research 2.
Underlaying concept idea
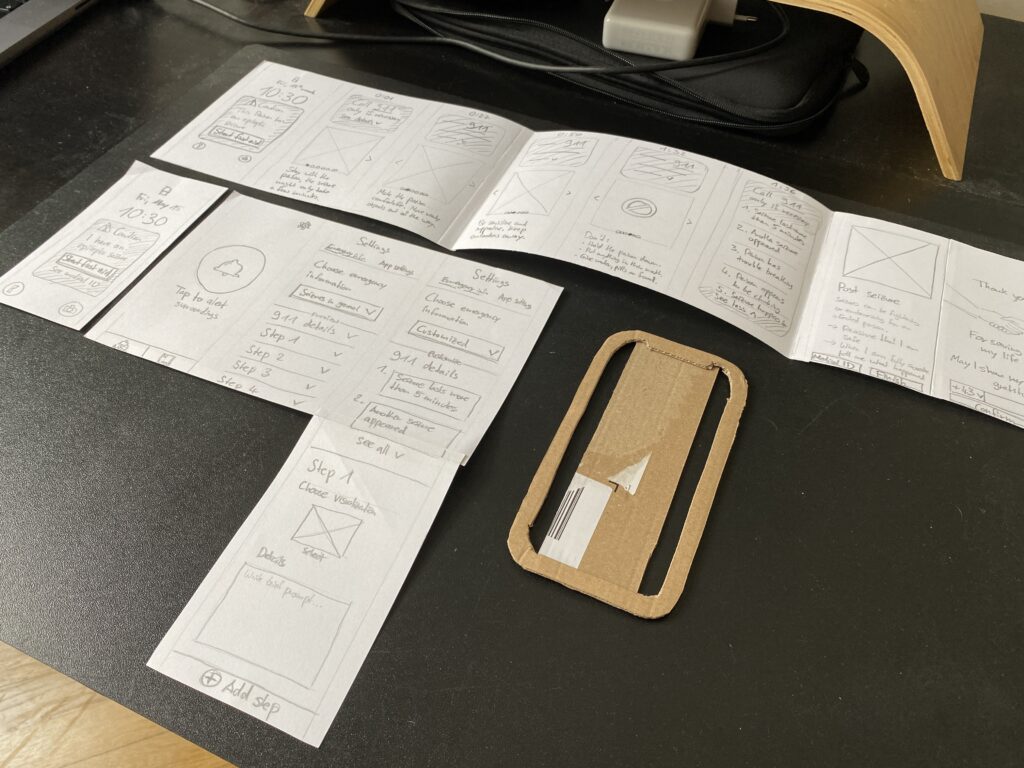
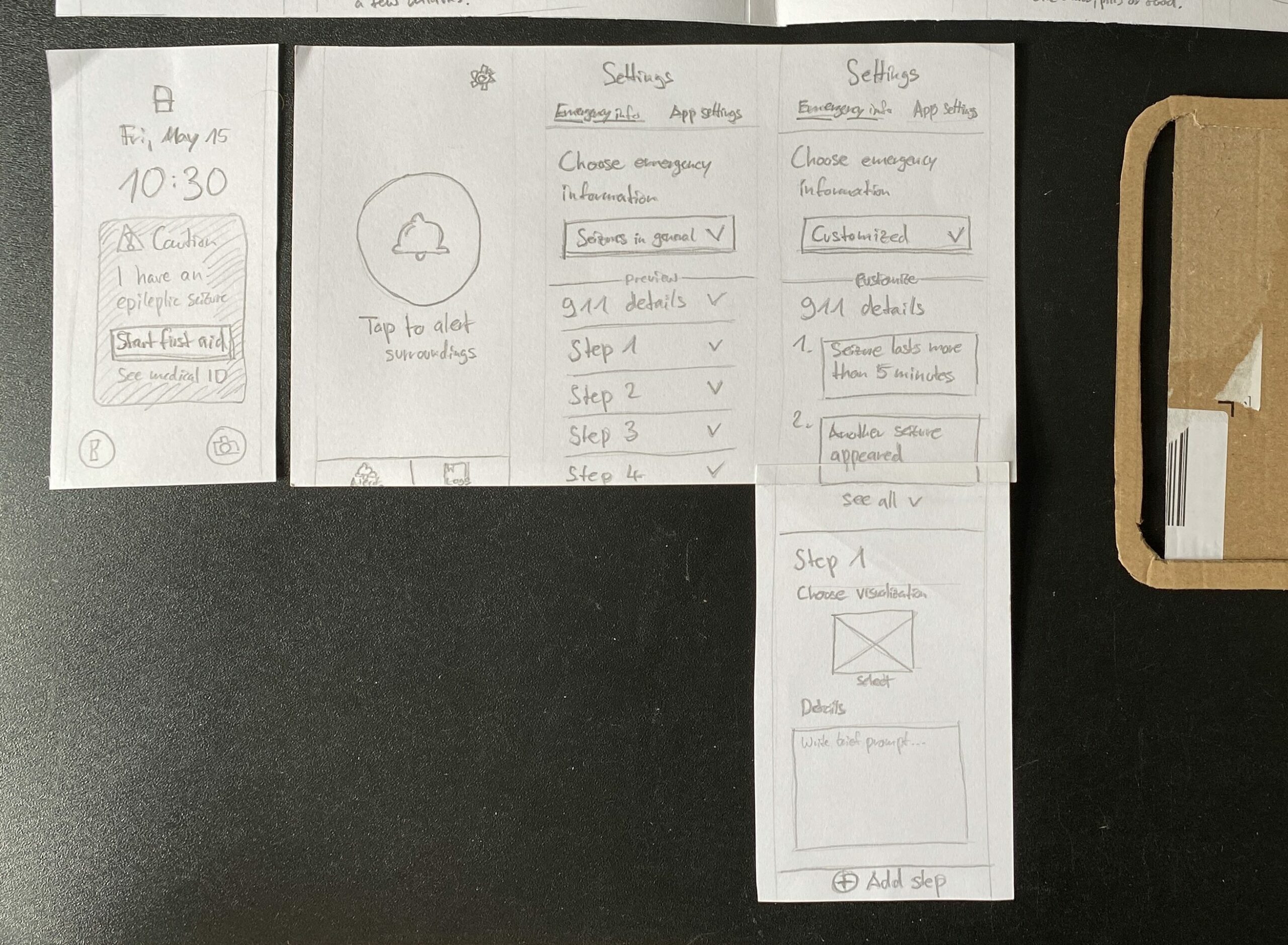
The present prototype represents a mobile app, which has to be manually activated by persons with epilepsy in case of emergency, if they notice an upcoming aura. Surrounding bystanders are then addressed by visual and auditory cues to pay attention to the smartphone.
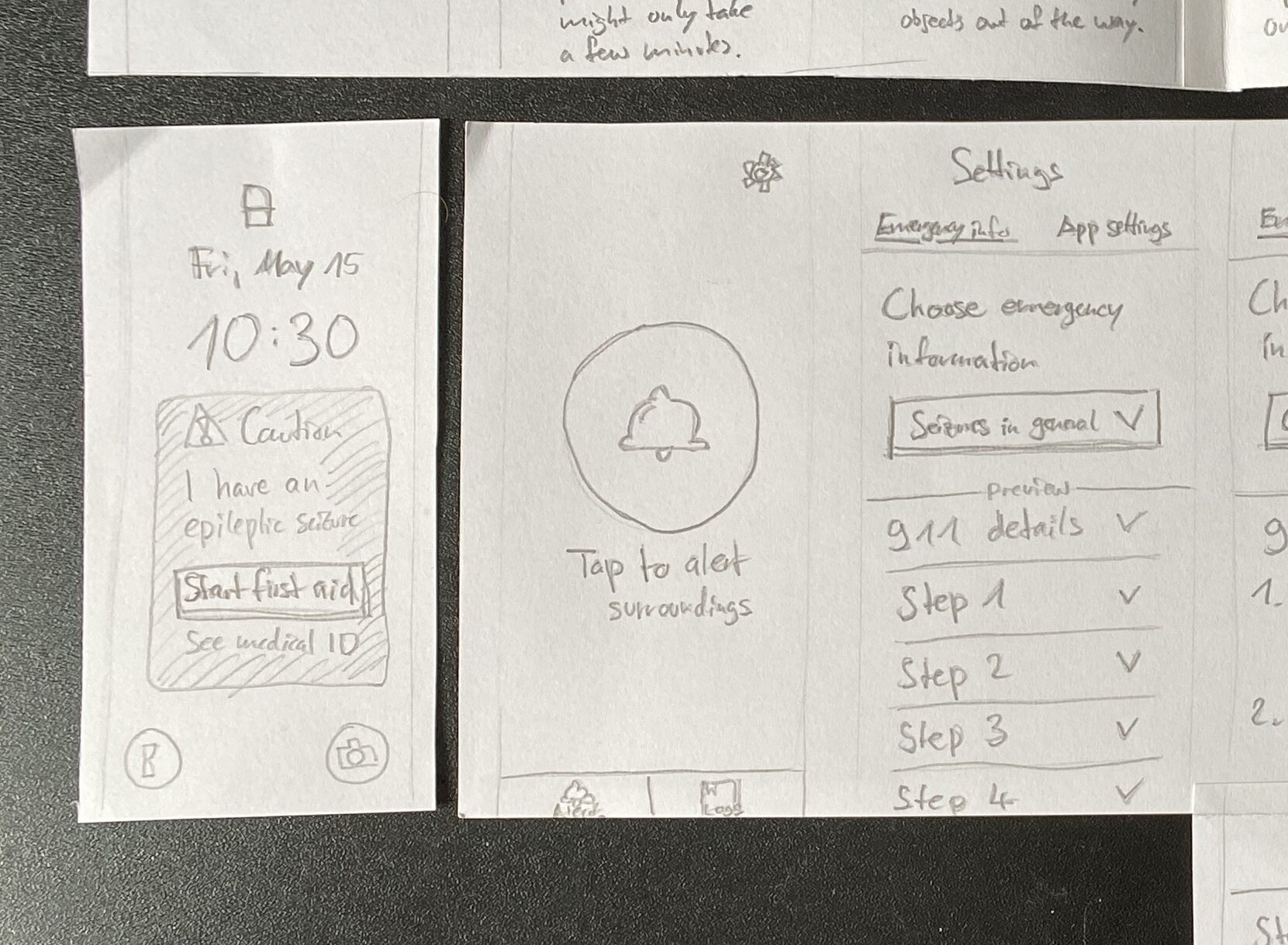
Having a look on the smartphone, bystanders are shown what’s the matter with the person and how to help. This follows a general set of emergency information which is applicable to nearly every type of epileptic seizure. Also bystanders receive information about when it is necessary to call an ambulance.
Advancement: Tailored emergency information
One of the biggest advancements might be the possibility to individually customize emergency information to an affected person’s specific condition. For this I added customizability to the app’s settings. Besides the general emergency information, which is set as a default, users are able specify the shown information steps to their own needs. A visual representation (picture, pre-made illustration etc.) and a short textual instruction in a few sentences can be chosen, and further steps can be added.
Advancement: Findability of medical ID
Another addition is a lock screen widget, once an alert has been activated by the person with epilepsy. In case of a locked phone, this piece helps to give an understanding and access to the first aid instructions as well as the medical ID. The latter is a often hidden feature on mobile operating systems, which gets more visible with the widget once an alert has been started.
Advancement: Expressing gratitude to bystanders
Lastly another advancement could be an extended way to end the app experience, when a seizure has been overcome: Besides communicating appreciation and recognition for the provided help, bystanders can optionally leave their contact details (e.g. a mobile number) for the affected person. Afterwards the rescued person is able to get in touch with its helper.
Auditory cues
As recommended by experts mentioned in the previous blog post the auditory level should play an important role as well, when it comes to the smartphone’s findability and support to follow first aid instructions. Obviously a paper prototype can not provide sound due to its material. This is where a, at least partly, digital component have to come in.
Next steps
Iterating and extending the paper prototype was quiet easy and quick. However its detail has to undergo refinements and the eventualities for various circumstances have to be considered. At this point it makes sense to transfer this haptic paper prototype into a digital prototype, to be able to add interactivity and sound.
As stated in blog post #11, the previous thoughts on my research journey were accompanied by doubts about the relevance and ability to make a serious contribution to the current state of research. To overcome these doubts, I allowed myself to dig deeper into the application areas mentioned that I could possibly focus on:
Ad Hoc First Aid Care Collaboration with the Public
Semi-Ad Hoc Care Collaboration During Transportation
Prior Education for Secondary Caregivers at Workplace/School
The „Ad Hoc First Aid Care Collaboration with the Public“ approach still interests me the most and is the area that is most in demand according to the experts1. This is why I started here.
Ad Hoc First Aid Care
In my research last semester, I realized that there are very few solutions when it comes to mobile applications and wearable technology. Some seem to be poorly designed, others are still in the concept stage, or seem to be no longer in operation. I looked at the following solutions in particular:
Seizure First Aide by the Epilepsy Foundation Minnesota2
Aura: Seizure First Aid by PT. Supremasi Astadaya Sentosa4
Medistat Seizure SOS by Saksham Innovations Private Limited5
For the evaluation, I made a comparison of how these solutions matched the results of my previous research. Early on, I realized that the only serious candidate I could consider, according to my findings and the experts‘ recommendations, was Aura: Seizure First Aid. By coincidence, the designers had the same idea for the app as I did and were inspired by the same content provided by the Epilepsy Foundation.6
Evaluation of Aura: Seizure First Aid
Aura: Seizure First Aid’s core features include the following:
This application addresses the following findings and recommendations as follows:
Conclusion
All in all, Aura: Seizure First Aid already meets the majority of my findings. The app is reduced to providing a general step-by-step approach to securing a person with epilepsy with a great user experience. The affected person has to start an alarm by simply tapping on the app. Their smartphone will then alert nearby bystanders to help and make a decision if an ambulance is needed. As soon as the seizure is over, the process ends with thanking the first responders for their help.
Because epilepsy comes in many different forms, it is highly individualized for each person. Participants in the study expressed a desire to provide bystanders with individually relevant information. Therefore, a mobile app could also allow users to customize the information displayed.
In addition, the general public rarely knows where to look for medical information about a person experiencing a seizure. Therefore, making the information more visible and accessible could be another addition. This could start on the lock screen of the phone.
Stories from people with epilepsy reveal a desire to thank bystanders after they have helped. Sometimes this is not possible because the person has not regained consciousness yet. Providing an extended way to contact helpers after a seizure could be another meaningful contribution.
Next steps
Taking into account my findings, the given app can be extended to meet the needs of a similar target group that values customizability when it comes to shared emergency information. This could be an approach where I can start working on a paper prototype.
Resources
Aehong Min, Wendy Miller, Luis M. Rocha, Katy Börner, Rion Brattig Correia, and Patrick C. Shih. 2021. Just In Time: Challenges and Opportunities of First Aid Care Information Sharing for Supporting Epileptic Seizure Response. Proc. ACM Hum.-Comput. Interact. 5, CSCW1, Article 113 (April 2021), 24 pages. https: //doi.org/10.1145/3449187↩︎
In the first semester I was able to get an insight into how epilepsy first aid could be supported by technology. To take things further, I would like to start with a brief reflection on how the findings and recommendations of this research can be further processed for a real-world prototype and what the next steps might be.
Thoughts on research journey
After taking some time to reflect, I began to doubt how my previous research could lead to a meaningful contribution, since this topic is very focused on a specific use case (emergency) for a specific disease pattern (epilepsy), and there seem to be some promising solutions already out there.
To come to a conclusion, I see three options on how to proceed:
Option 1: Continue with my topic and start prototyping ideas. This would mean no more research than usual.
Option 2: Stay close to my previous research, but eventually choose a different use case or project approach. If necessary, look for similar areas where my research knowledge can be applied. In case of a change of direction, this could mean additional research.
Option 3: Completely change the topic. This would mean the highest amount of (new) research needed and could possibly lead to time constraints.
Weighing the options, a path between options 1 and 2 seems to make the most sense: The first step would be to recall my research findings (pain points, recommendations, etc.).
Next, I should try to evaluate how existing solutions align with what I have learned about the pain points of the target audience and the recommendations of the experts (option 1) to see if there is room for improvement or if a custom concept is even needed.
At the same time, I should be open to following other project ideas if the room for a serious contribution is too small or non-existent (option 2).
Given that this research phase is focused on prototyping, it is of course important to gain more insight into users and stakeholders.
Project approaches to follow
During my previous research, I found expert advice on areas of possible projects1. These include:
Ad Hoc First Aid Care Collaboration with the Public
Semi-Ad Hoc Care Collaboration During Transportation
Finding a Person in Charge & Care Information Sharing When Utilizing Public Transportation
Seizure Monitoring & Information Sharing While Driving
Prior Education for Secondary Caregivers at Workplace/School
After a second look at what I’ve found out, I want to start evaluating existing solutions for „Ad Hoc First Aid Collaboration with the Public“, which according to the experts is the area that is most in demand. At the same time, it has my greatest interest.
Resources
Aehong Min, Wendy Miller, Luis M. Rocha, Katy Börner, Rion Brattig Correia, and Patrick C. Shih. 2021. Just In Time: Challenges and Opportunities of First Aid Care Information Sharing for Supporting Epileptic Seizure Response. Proc. ACM Hum.-Comput. Interact. 5, CSCW1, Article 113 (April 2021), 24 pages. https: //doi.org/10.1145/3449187↩︎
Over the past three months, I have primarily conducted literature research on the overall topic of First Aid Assistance for Chronic Diseases. During this process, this topic has evolved in diverging and converging research phases, becoming more and more detailed over time. At this point I would like to briefly recapitulate what I have learned so far.
Research development
With the announcement of my research topic, I got to know better what first aid and the chain of survival means. I also got a great impression of what interactive first aid applications exist and what areas they cover.
In the beginning, I started to keep the topic very rough, which allowed me to discover things. To understand what first aid consists of, I drew a bigger picture of the different aspects. I also had a first idea of what types of chronic diseases could be considered. Very early on, I realized that I was interested in the specific context of sudden emergencies.
As I delved deeper into the variety of chronic diseases, I discovered types that were suitable and less suitable for my research. I also learned the difference between diseases, symptoms and disease events. The candidates were cardiac arrhythmia, diabetes and epilepsy. What makes epilepsy different from the others is that not every seizure is life threatening. I found this interesting. That is why I decided to pursue this path in my research.
I looked deeper into epilepsy first aid and found a general approach that can be applied to any type of epileptic seizure: Get the person into a safe state and recognize when it is time to call an ambulance. So there is a difficult decision-making process involved.
I was lucky enough to find this very valuable scientific article that describes the current state of research for my central research question: How can we use technology to support first aid? This helped me immensely to understand the criteria that need to be considered, the pain points of people with epilepsy and their families, and recommendations for future technologies to address these issues.
In my search for tools and methods as a starting point for project work, I came across this scientific paper explaining and categorizing different design approaches. It highlighted the possibilities and limitations of design in the strict field of healthcare, which helped me to evaluate where to place a potential project.
Finally, I tried to find out more about untrained first responders who have experience helping a person with epilepsy. This turned out to be very difficult, so I tried to make assumptions about their perspective by studying seizure first aid stories. If further research on this is unsuccessful, I would need to gather information using other (empirical) methods.
Outlook
From this point of research, the next steps would include the following:
Gain greater insight for all stakeholders through additional (user research) methods
Further evaluate existing solutions
Consolidate insights, findings and other information into an initial concept
One of the research questions of my work hasn’t received much attention: „What challenges, needs, and expectations do first responders face?“
In order to include the perspective of first responders, I conducted a literature and web search to see if there was already information available. In terms of time spent, the search so far has been quite difficult. It seems that there is very little information about the experience of untrained first responders in the public area.
However, I was able to find seizure first aid stories published by the Epilepsy Society in the UK. As part of National Epilepsy Week in 2019, they are running a campaign called #seizuresavvy. People were asked to share their first aid experiences, both good and bad.
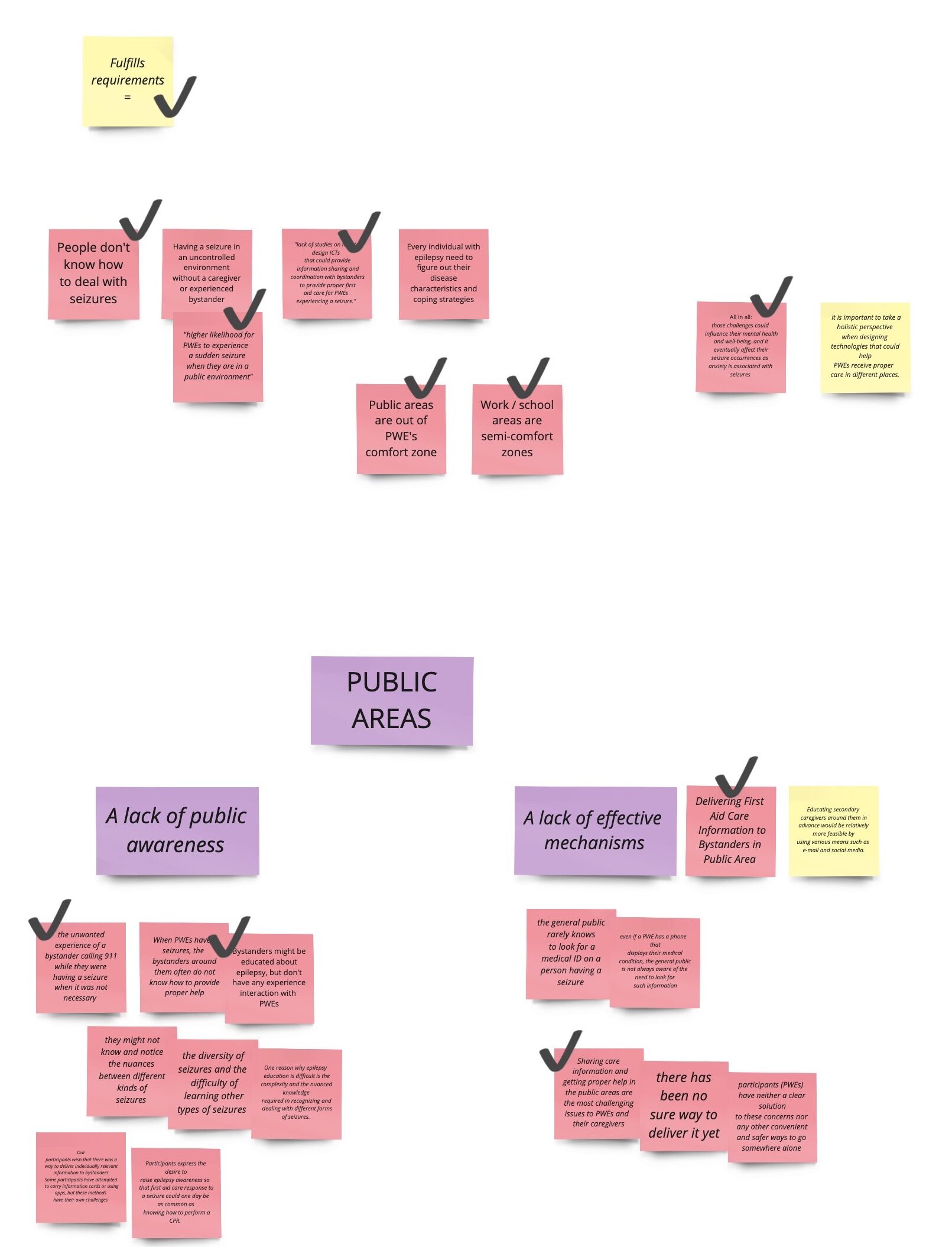
By studying these stories, I tried to draw conclusions about the challenges, needs and expectations of first responders. The people with epilepsy (PWEs) who contributed their experiences were Vicky, Michael, Chloe, Kas, Tim and Tom. Their stories tell how and who took on the role of first responder. I extracted the information for these three aspects and grouped them into the following five categories.
Education, training, awareness
Effective education and training for first responders is critical, as illustrated by several scenarios involving people experiencing seizures. Rapid decision-making and action are essential in critical situations, emphasizing the need for first responders to seek help quickly and make informed decisions.
There is also a clear call for increased public awareness and education about epilepsy to prevent misunderstandings and ensure appropriate responses in emergencies. Basic first aid skills, such as placing people in the recovery position, can have a positive impact on well-being, highlighting the importance of even simple interventions.
However, challenges exist, including potential misconceptions about seizure first aid, such as the common misconception of placing objects in the mouth. The unpredictable and potentially life-threatening nature of seizures, especially in cases of unstable epilepsy, further complicates the role of first responders.
Advocacy for awareness campaigns and education initiatives is essential to address gaps in public perception and understanding of epilepsy. Individuals such as Chloe and Paula advocate for broader societal awareness, support and understanding, emphasizing the need for education among various groups, including teachers and first responders. The lack of awareness of specific epilepsy conditions, such as photosensitive epilepsy, poses challenges for individuals like Chloe and highlights the importance of comprehensive education and resources.
Communication
Effective communication plays a critical role for first responders in emergency situations. In one scenario, a five-year-old niece had to effectively communicate the emergency to get help from neighbors and emergency services, highlighting the importance of clear and concise communication, even in difficult circumstances.
Vicky probably expected her niece to communicate the situation to the emergency services, underscoring the need for effective communication to ensure a rapid response. In a different context, Tim faces the challenge of recognizing the onset of a seizure, particularly during activities such as running, where rapid communication to bystanders and their response is critical.
Tim’s experience also highlights another aspect of communication challenges – the lack of opportunity for acknowledgement. Despite receiving first aid, Tim was unable to express his gratitude and thanks to those who helped him during the incident. From the first responder’s perspective, they must assume that they will not receive conscious recognition from the individual. This underscores the importance of providing opportunities for individuals to recognize and appreciate the help they receive, thereby contributing to a sense of gratitude and recognition within the community.
Structural circumstances
The structural circumstances surrounding first responders highlight crucial aspects of recognition, support, and challenges faced by individuals like Chloe. As a student, Chloe expects recognition of her epilepsy as a legitimate medical condition and anticipates knowledgeable and supportive responses from teachers and first responders during seizures.
However, stigma poses a significant challenge, as Chloe’s primary school teacher doubts the authenticity of her seizures based on her appearance, and secondary school first responders refuse to help because of the perceived violence of seizures. This underscores the importance of addressing misconceptions and promoting understanding to eliminate stigma in educational and healthcare settings.
Establishments such as supermarkets are also implicated in these structural circumstances. There’s an expectation that such places should have policies and procedures in place to support people experiencing seizures, ensure their safety and prevent them from being left alone after an episode.
The findings underscore the critical need for increased education and training for teachers and first responders. This includes recognizing the type of seizure a student, teacher, employee or customer is having and responding appropriately.
Supportive environment
Creating a supportive environment for persons with epilepsy (PWE) involves a combination of knowledge, training, and understanding of different circumstances.
For example, Vicky teaches her niece about seizure response and emphasizes the importance of preparedness.
In Michael’s case, there’s a potential need for emergency response training for his family, especially Paula, given the unpredictable and severe nature of his seizures. This highlights the importance of ongoing education and preparedness for families living with epilepsy.
Chloe needs a supportive environment at school, where teachers and first responders understand her condition and offer help without stigma. This highlights the need for awareness and understanding in schools to create an inclusive atmosphere for persons with epilepsy.
Response time
The importance of response time is a common thread in several scenarios involving first responders. Vicky’s niece faced the challenge of acting quickly in a time-sensitive situation when Vicky was about to have a seizure, highlighting the critical nature of timely responses.
For people like Michael, getting help in a timely manner when he is having a seizure is critical because of the potential severity of his condition. The expectation is that those around him can respond quickly to provide the necessary support.
In another context, a store assistant became a first responder in a public setting and faced the challenge of responding to a medical emergency involving a tonic-clonic seizure. This highlights the need for individuals in public spaces to be prepared for timely responses to such situations.
It also highlights the need for support during the recovery phase, as seen with Kas, who requires assistance in regaining consciousness and ensuring a safe environment following the seizure. This further emphasizes the time sensitivity not only during the seizure itself, but also in providing support in the aftermath.
Conclusion
Overall, finding experiences from untrained first responders in public settings has been difficult. It is easier to find experiences from persons with epilepsy and those around them than from strangers.
It is questionable whether a more in-depth literature and web search would reveal more information. It could be assumed that previous research and resources do not cover the experiences of untrained bystanders if they are not known or it is not important for them to share their perspective. In order to include their perspective, it may be necessary to reach out to them by initiating an open call or something similar.
Gaming has been increasingly used in therapy as a tool to improve physical and mental health. It has been found to be effective in treating a wide range of mental health conditions, including depression, anxiety, and post-traumatic stress disorder (PTSD). But it has also proven useful in motivation people to use physical therapy, as can be seen in [1].
[1] Gaming being used as a playful way to motivate patients to actively take part in therapy sessions.
Regarding physiotherapy, video games offer dynamic and interactive exercises that target specific motor skills and promote physical rehabilitation. In this context, the word exergaming gets used. Of special interest is the field of pediatric care/therapy because especially for children, video games transform therapy sessions into engaging adventures, motivating them to actively participate in their treatment.
Impact of video games
Gaming in therapy isn’t just about entertainment; it’s about leveraging interactive digital experiences to promote health and well-being. From physiotherapy to pediatric care, video games are being integrated into treatment protocols to engage patients, enhance rehabilitation outcomes and foster a sense of empowerment. They can also provide an escape for patients, where they are temporarily transported into alternative worlds. Though escapism should always be handled with care, these moments can reduce the pain felt and bring joy to patients.
Benefits
Enhance the experience for the patient Video games provide a new and novel approach to keep patients interested.
Personalized treatment Digital treatment methods such as video games can be highly customizable and easily replicable.
Real-time feedback Patients get instant feedback, e.g. regarding their posture, and then can act accordingly. Also, for some patients visual feedback can be more beneficial than verbal instructions.
Challenges
Accessibility and cost There is a certain amount of investment cost required to set up the hardware. Also, software, especially if it needs to be made completely new, can be quite expensive.
Applicability Treatment methods need to be applicable for a wide range of different age groups and patients.
Balancing gaming and treatment The treatment part should always remain the main focus. Gaming should only help to enhance, not overtake, the therapeutic objectives. Also, it should only be used when there is a specific reason or need to do so. As several studies have shown, the physical impact is very similar to traditional treatment methods. The advantage therefore lies in the novelty, joy and motivation this process can bring.
Technical implementation
From the articles I have gathered, there are many ways how to realize this idea of gaming therapy technically. One method often mentioned is the Wii gaming console which can be controlled by motion gestures via controller or some games can be controlled via balance board. But also head mounted virtual reality displays can provide useful, such as the Meta Quest, Sony PlayStation VR or the HTC Vive (among many others).
Summary & conclusion
Gaming in therapy represents a paradigm shift in patient care, offering novel approaches to rehabilitation and promoting overall well-being. As we continue to explore the therapeutic potential of gaming, it is essential to embrace innovative solutions that enhance patient outcomes and foster a culture of holistic healthcare. Gaming in this sense would not be seen as a replacement of traditional treatment methods, but as an enhancement to existing treatment structures.
While searching for a suitable practical methodology for this research project, I came across a scientific paper for a Design Research Society conference in 2018, written by Dr. Erez Nusem, University of Sydney. The paper gives an overview of different design approaches for healthcare, which can be applied not only to UX and interaction design, but also to industrial and social design.
When bringing research into project work, these approaches can help to define the relationship between the prescribed outcome and the constrained context, as well as the extent to which design can or should have an impact when talking to stakeholders.
Design as an human-centered approach
Healthcare systems are becoming increasingly conscious of the quality of care delivered, nevertheless the majority of innovation in the realm of healthcare has been focused on products and services. These technology-driven innovations treat medical staff as the primary stakeholder and do little in the way of improving the quality of care for patients. As a human-centered approach, design offers a method for holistically exploring problems, meeting stakeholder needs, and has been established as a means of driving innovation.
Systematization
The author categorizes four design approaches and places them on a coordinate system that shows the relationship between the amount of prescribed and constrained context. This emphasizes the impact of designing for healthcare, where precise boundary conditions do exist.
Interpreting design opportunities in healthcare (synthesis from Nusem, Wrigley & Matthews, 2017; Mosely, Wright & Wrigley, 2018)
Design approaches
Result-centered design (simple)
Description
Design follows ‘the rules of the game’, concentrating on design conventions, customs and habits, and the set ways of working within a field (e.g. concentrating on the user and designing from their perspective).
Example
As articulated directly by the staff, previous ultrasonic scanners were very immobile and heavy. Philips designed a machine which could easily be moved around a patient. The process based on observation and analysis of current devices in use.
Requirements
Basic understanding of design.
Problems are easy to identify and articulate.
A deep sense of empathy is not required.
Suitable design scenarios
No consideration of workflow and processes in newly designed environments.
Lack of standardised procedure for training and use of equipment.
Lack of standardised platform in hospital for collecting and storing patient data.
Situation-centered design (complicated)
Description
Design follows ‘the rules of the game’, concentrating on design conventions, customs and habits, and the set ways of working within a field (e.g. concentrating on the user and designing from their perspective).
Example
A group of designers worked on improving the information exchange between nurses in shift changes, which has been incomplete and resulted in unsatisfied patients. As a result nurses were advised to share information in front of patients, which increased quality of information transfer between all stakeholders and shorter preparation time for nurses.
Requirements
High design competency required, since design criteria can be difficult to define.
Context needs to be explored holistically.
Suitable design scenarios
Patients with undiagnosed conditions which are discovered through unrelated treatment.
Outdated workflows that have evolved over time, with no deliberate design.
Suboptimal experience in waiting rooms with issues around long wait times for patients.
Subject-led design (complex)
Description
Design is concerned with the process and development of new ways of working which are imposed upon a problem (e.g. reframing the design problem to develop something new).
Example
CT scanners require patients to remain still for as long as the lengthy exposure takes. Instead of increasing the imaging source‘s power, causing a higher dose of radiation, designers came up achieving a more enjoyable experience while scanning through changing the hospital‘s environment.
Requirements
Being open-minded to undefined outcomes.
High degree of empathy and understanding of stakeholders and challenges.
Suitable design scenarios
Staffing issues (e.g., understaffed due to low retention), meaning patients often need a return visit following diagnosis.
Patients with visible medical products are self- conscious.
Prolonged stay in sterile environments, with minimal interaction with other humans.
Design for innovation (chaotic)
Description
Design is revolutionary and disruptive, where the designer explicitly aims to redefine the field (e.g. the entire problem and solution are reconceptualised).
Example
Medicial errors are often caused of incorrect usage of medical devices due to a technological design focus. Designers who consider users and usage scenarios are able to achieve a seamless user experience, which benefits ease of use and shortens learning time for medical staff.
Requirements
Being open-minded to leave conventional paths and practices.
Being open-minded to undefined outcomes.
Overall holistic perspective required.
Masterful design competency, facing ambiguity without pre-existing solutions.
Suitable design scenarios
Lack of channels for patients both pre and post-care (e.g. initiating care and discharge) to be engaged in their care.
Desensitised staff which see patients cases rather than individuals.
Services are not value-driven and do little in the way of ensuring optimal patient outcomes.
Insights
Regarding my research, I’d like to classify my research project between situation-centred design and design for innovation regarding the following aspects:
Situation-centered design
The context needs to be explored holistically, as it is emergency relevant, it must work for different contexts.
The solution can be narrowly prescriptive, optimizing the few existing solutions.
Design for innovation
There is a lack of existing solutions.
Given new technologies and devices, the outcome could be anything.
A holistic approach to users and context of use, as suggested by the authors, is needed: Taking into account the attribution of epilepsy stigma, such as the visibility of seizures and cultural perceptions, as well as the different symptoms of epilepsy, as people with epilepsy often experience different individual and social challenges depending on the severity of their symptoms.
Resources
Nusem, E. (2018) Design in Healthcare: challenges and opportunities, in Storni, C., Leahy, K., McMahon, M., Lloyd, P. and Bohemia, E. (eds.), Design as a catalyst for change – DRS International Conference 2018, 25-28 June, Limerick, Ireland. https://doi.org/10.21606/drs.2018.318
Many times during my research, I have come across the importance of ethical considerations for the use of VR (both as a consumer product and a medical instrument) and about the usage of modern technology in healthcare in general. In this blog post, I want to delve deeper into some of the challenges and important lessons regarding ethics in this environment.
Using VR and modern digital technology in treatment settings introduces a host of ethical considerations. One of the primary concerns revolves around patient privacy and data security. With the collection and utilization of sensitive health information through digital platforms, ensuring robust safeguards against data breaches and unauthorized access becomes paramount. Health information is sensitive information. When protection is not set up correctly, many people can be compromised, as can be seen in [1], which is a list of the 14 biggest healthcare data breaches
Another ethical consideration is about informed consent and patient autonomy. As patients engage in VR therapy or digital therapeutics, they must be fully informed about the nature of the treatment, its potential risks and benefits, and any alternatives available. Furthermore, ensuring that patients have the capacity to provide informed consent, especially in cases involving vulnerable populations or individuals with diminished decision-making capacity, is essential. Especially regarding new technologies, patients may not know about potential risks/benefits and may be ill-informed – the goal of the professional has to be to inform the patient about these factors.
Furthermore, the equitable access to VR therapy and digital interventions raises concerns about healthcare disparities. As these technologies become more prevalent in treatment settings, ensuring equitable access across diverse socioeconomic and demographic groups becomes imperative to prevent exacerbating existing healthcare disparities. Another aspect to keep in mind are the biases of the professionals creating these services, as talked about in [2] or written about in [3] and [4]. A diverse team of people with different backgrounds can ensure that all facets are addressed and that no group of people is disadvantaged in any way.
[2] An interesting discussion about the ethics of VR and its usage as a consumer and medical product.
Addressing ethical challenges requires a multifaceted approach that encompasses technological, regulatory, and ethical considerations. Implementing robust data protection measures, such as encryption protocols and secure storage systems, can help safeguard patient privacy and mitigate the risk of data breaches.
Furthermore, integrating informed consent processes into VR therapy and digital treatment platforms empowers patients to make informed decisions about their healthcare journey. This involves providing comprehensive information about the treatment modality, including its potential risks, benefits, and alternatives, in a clear and accessible manner.
Promoting transparency and accountability within the healthcare ecosystem also plays a crucial role in addressing ethical concerns. Healthcare providers and technology developers must adhere to ethical guidelines and standards of practice, ensuring that patient interests are prioritized throughout the treatment process.
Summary & conclusion
As we navigate the evolving landscape of healthcare technology, the ethical considerations surrounding VR therapy and digital interventions will continue to shape the future of patient care. As designers, embracing a culture of ethical reflection and continuous improvement is essential to foster trust and integrity within the broader community.
Looking ahead, advancements in artificial intelligence, machine learning, and immersive technologies are most likely about to revolutionize healthcare delivery and patient outcomes. However, as we embrace these innovations, it is imperative to remain vigilant in safeguarding patient rights, promoting equitable access, and upholding ethical standards. In conclusion, navigating the ethical considerations associated with VR therapy and modern digital technology in healthcare requires a collaborative effort grounded in principles of transparency, accountability, and patient-centered care.
References used in this article and for research
The notes under the links are mostly for myself, in order to have an organised overview over the content of each source.
Referring to the authors‘ suggestions for innovative approaches in the previous blog post, I conducted further divergent research on existing solutions in the following areas:
Ad Hoc First Aid Care Collaboration with the Public
Semi-Ad Hoc Care Collaboration During Transportation
Prior Education for Secondary Caregivers at Workplace/School
Research criteria
Due to the fact that the authors propose innovative solutions, I noticed a general lack of existing solutions during my research. Looking at the identified pain points that people with epilepsy (PWE) face, I assumed that bystander first aid in public was the most desirable and interesting area. Also, the solutions for this topic are more tangible. I came up with the following criteria to search for:
A solution must work for all types of seizures in general, as they are very individual and the differences are not well known.
A solution must provide information about when to call 911. This is not always the case when a seizure occurs.
A solution must guide untrained bystanders to provide first aid in an emergency, as they may be able to place a person in a safe condition to prevent injury.
A solution must make emergency information clearly visible and accessible to bystanders and medical professionals, otherwise it may be overlooked.
Mixed reality
HoloCPR
Although this solution addresses cardiopulmonary resuscitation (CPR), the authors propose to adapt this concept to epilepsy. HoloCPR is a mixed reality interface that assists bystanders in providing first aid by providing visually augmented user guidance. The developers, associated with UC San Diego – Jacobs School of Engineering and UC San Diego Design Lab, found that this technology can reduce the response time and ease of first aid actions compared to using a tablet application.
Other than this solution, I have not been able to find a virtual reality, augmented reality or mixed reality solution that is specifically tailored to epilepsy. Furthermore, for this concept to work, mixed reality devices need to be further integrated into our daily lives, as seizure emergencies are unpredictable and bystanders need to have the technology with them.
Mobile apps
Aura: Seizure First Aid
Aura is an app designed to help people with epilepsy by alerting their environment and caregivers when a seizure is imminent. Other key features include step-by-step seizure first aid instructions, access to medical IDs, live location sharing, and tracking events in seizure logs.
In doing so, the app provides an all-in-one solution that attempts to cover multiple application areas.
Medistat Seizure SOS
Medistat Seizure SOS takes a similar approach. It is designed to empower epilepsy patients by alerting those around them to seek help: When a seizure occurs, the app notifies nearby bystanders and provides them with audio instructions to effectively provide first aid to the person with epilepsy. Opening the app automatically sends alerts and SMS messages to pre-defined emergency contacts. The app actively and continuously tracks the live location, ensuring that caregivers are constantly updated on the individual’s exact whereabouts.
However, based on app store numbers and reviews, this app appears to be under-utilized.
Wearable devices
MyID
MyID allows you to store your entire medical profile, including emergency contacts, vital signs, medical images, and more. This online profile is linked to a MyID wristband that allows medical professionals and bystanders to access detailed medical information via a QR code.
Compared to traditional medical ID wristbands, where health information is engraved on a small surface, MyID allows users to store an unlimited amount of information in the digital space. However, these devices can be overlooked by untrained bystanders who are the first on the scene in the event of a seizure emergency.
Dialog
Dialog is a concept for an epilepsy aid that focuses on seizure monitoring and detailed reporting. It is a wearable module that can be attached to the skin either by a transparent adhesive or by a watch-like clip. It is also capable of providing early warnings so that a person can prepare to move to a safe state, and a separate bystander app provides step-by-step instructions on how to help a person in an emergency.
This technology concept is beneficial for the end user, who can decide where to wear the module and how visible it is. On the downside, it requires bystanders to install a separate app, which prevents most people in public from acting as first responders.
Conclusion
As I researched existing solutions, I realized how few there were. These examples give a sense of where the industry might be today.
Regarding the Indiana University Bloomington research mentioned in previous blog posts, evaluating existing solutions using the pain points from the research can reveal optimizations.
This blog post is a continuation of the previous post #05, where I talked about the definition and explanation of various terms surrounding the topic of immersion therapy. In this second part, I want to go deeper into the advantages and disadvantages and specific use cases for these treatment methods. This will hopefully deepen my understanding of this subject and which elements are or are not important.
Advantages and disadvantages of this treatment method
As mentioned in previous blog posts, this type of therapy can be used to treat both physical and mental health problems. As a side note, I found that the internet provides many resources when it comes to the treatment of mental health problems but less so for physical problems. In the upcoming section, I will talk about advantages and disadvantages for both mental and physical problems, as these often times overlap and apply to both.
Let us discuss briefly what the distinct advantages of this digitized approach of therapy is, over more traditional ways.
It is a very safe and controlled environment. People can be gradually exposed to their fears/problems/anxieties. The therapist can fully control the level of exposure and also monitoring devices, e.g. for the heart rate, may be utilized to gather information. Furthermore, the patient can rest assured that they can end or pause the treatment whenever they feel overwhelmed.
Be more engaging and interactive experience. For example, compared to traditional talking treatments, the patient feel more immersed and connected to the experience. This helps with the efficiency of the treatment and can also be useful when dealing with patients with a low attention span or motivation, such as with children. Furthermore, VR is shown to be able to reduce the pain levels experienced by patients. It can help to break or alleviate a negative feedback loop caused by pain, dizziness and fatigue.
It can be time- and cost-efficient. A VR setup can be quite inexpensive and certain scenarios may be reused multiple times. Also, the treatment can easily be done in a simple room. Comparing this to e.g. treating the fear of flying where one would need to somehow simulate a flight or go flying, the ease of use becomes apparent.
The results produced by this method seem to be long-lasting and very positive according to several studies done. However, even though this sound positive, more research is needed. Most research done thus far is on phobias and PTSD, its use for other problems still needs to be thoroughly researched.
Treatment may be administered remotely. Some patients may not be able to leave their homes. VR therapy could be used to deliver training/therapy materials to patients anywhere.
Of course this type of treatment method also has disadvantages and problems, such as:
Technical aspects can prove difficult. Such as the initial setup cost, bugs, hardware problems and also the need to create programs/levels/scenarios for the specific treatment. This takes time and money.
Therapists need to be trained to utilize this tool. The adoption of VR technology as a therapy method is slow, and many mental health professionals are also not trained to work with it. This is also a problem here in Austria, where very few places (hospitals, etc.) actually work with and support it.
Patients may not feel open to this treatment approach and not accept it. Instead seeing it a simple gimmick with no real usage.
Let us talk very quickly about why exposure therapy works. There are several ways how it functions and creates positive effects:
Habituation – meaning that through exposure, people can become accustomed to their fears and decrease their reaction to the object/situations which create the fear.
Extinction – similar to habituation. Previous (negative) associations with objects/situations can be weakened or even replaced with positive emotions through exposure.
Self-efficacy – patients learn that they are strong enough to handle their fears on their own and confront them forthright.
Emotional processing – describes the process in which patients change their beliefs about objects/situations/activities/… and attach new, more realistic beliefs and emotions to them.
VR can be used to target areas in the brain responsible for pain processing and help regulate them and reduce the pain felt. For this reason, it can be used to treat several forms of chronic pains.
Summary & conclusion
Again, since this blog post is getting kind of long, I will continue and finish this subject in blog post 7 – part 3. There I will go into further detail regarding specific use cases for immersion therapy.
In this blog post, advantages and disadvantages were discussed. It is important to look at both sides and have a realistic view about this new form of therapy to be able to best use it. Furthermore, a brief overview over why this form of therapy works has been given.
References used in this article and for research
The notes under the links are mostly for myself, in order to have an organised overview over the content of each source.