In order to validate my first prototype idea, our lecturer Birgit Bachler encouraged me to get in touch with a nearby interest group in Graz: Institut für Epilepsie IFE.
In the course of a 45-minute meeting, I was able to demonstrate my paper prototype on site and ask questions about my research results and the experience of my contacts. Regina and her colleague were very interested in my project.
Starting an alert to bystanders
Speaking from experience, Regina and her colleague told me that working with sensors to detect an aura before a seizure is much more feasible for a person who is going to have a seizure. Many people do not recognize the onset of a seizure, and when they do, it takes too long to manually activate an alert in the open app. Examples of such inputs are Fall Detection and Brainwave Detection.
Visibility of wearable devices
Some of the studies I found suggested making electronic devices less visible. Contrary to what I found in my literature review, Regina and her colleague never met people who were reluctant to wear conspicuous devices for fear of stigmatization. Instead, they are happy to have them.
Advancement: Expressing gratitude to bystanders
Regina and her colleague responded positively to my planned feature that would allow people to reach out to their supporters by leaving contact information. They had never seen such a personal approach in any device and thought it was a nice idea for human relations.
Advancement: Tailored emergency information
Throughout the conversation, we talked about different types of epileptic seizures, especially those that are not really addressed by technological solutions. They explained that tonic-clonic seizures are most associated with spasmodic movements, but seizures that are expressed through confusional states are often overlooked. When I explained my idea for an individualized feature, Regina and her colleague were excited about the idea: Allowing people with epilepsy to view emergency information tailored to their own form of epilepsy could potentially provide more targeted first aid.
Choice of medium
When I asked my contacts about an appropriate medium for my endeavor, they confirmed that a mobile application is indeed appropriate from their point of view. It doesn’t require anything more than a smartphone, which many people already have. Also, most of the people they treat are used to the existing technological solutions, which in most cases include a smartphone. In fact, they gave me a printed version of a seizure care pass where people can write individual instructions for their own condition. The downside is that this document can easily be overlooked by first responders and the content is less appealing to read.
Log feature
When Regina and her colleague mentioned that some users would appreciate having a log where they could see past incidents, I showed them the feature in my paper prototype.
Conclusion
In the end, I was provided with a lot of informational material, a warm handshake, and the possibility to always reach back to Regina and her colleague. Overall, this step was really valuable to me and it did not take much effort to get quick and useful feedback, even when using a low-fidelity paper prototype to demonstrate ideas.
Next steps
Next, I would like to incorporate the feedback I received from the Institut für Epilepsie into the development of my prototype and possibly contact them if I need more expert opinions.
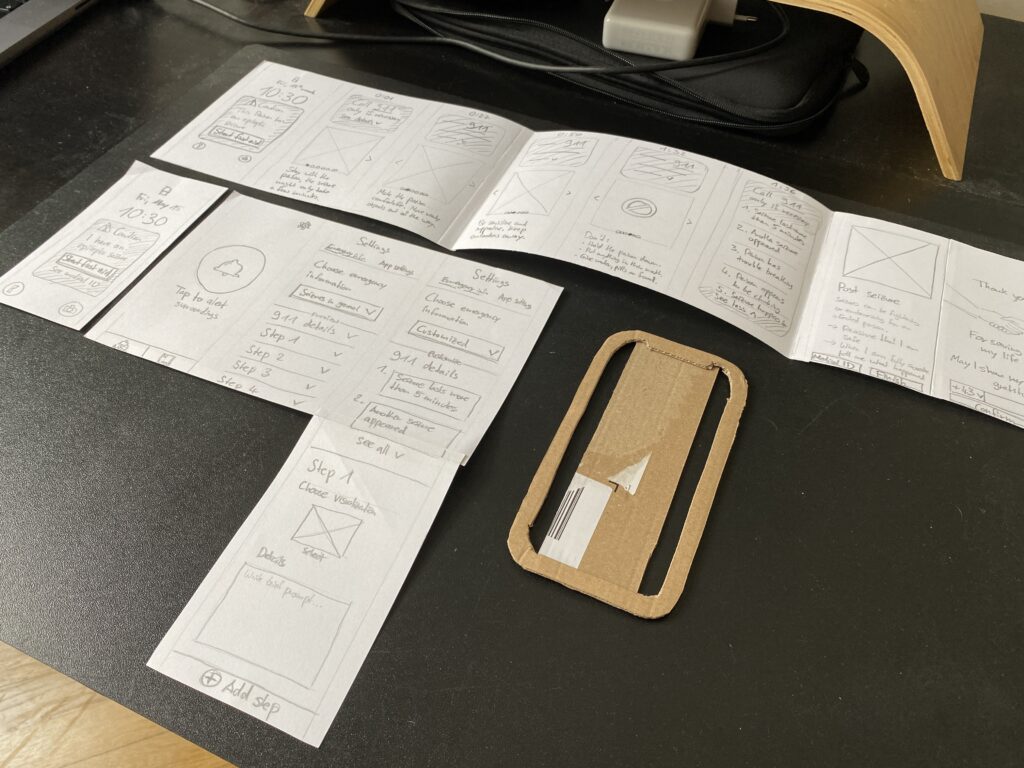
With regards to the example of Aura: Seizure First Aid mentioned in the last blog post, I iterated on a paper prototype regarding „Ad Hoc First Aid Collaboration with the Public“. This prototype had its origin in an exercise at the very beginning of the course Design & Research 2.
Underlaying concept idea
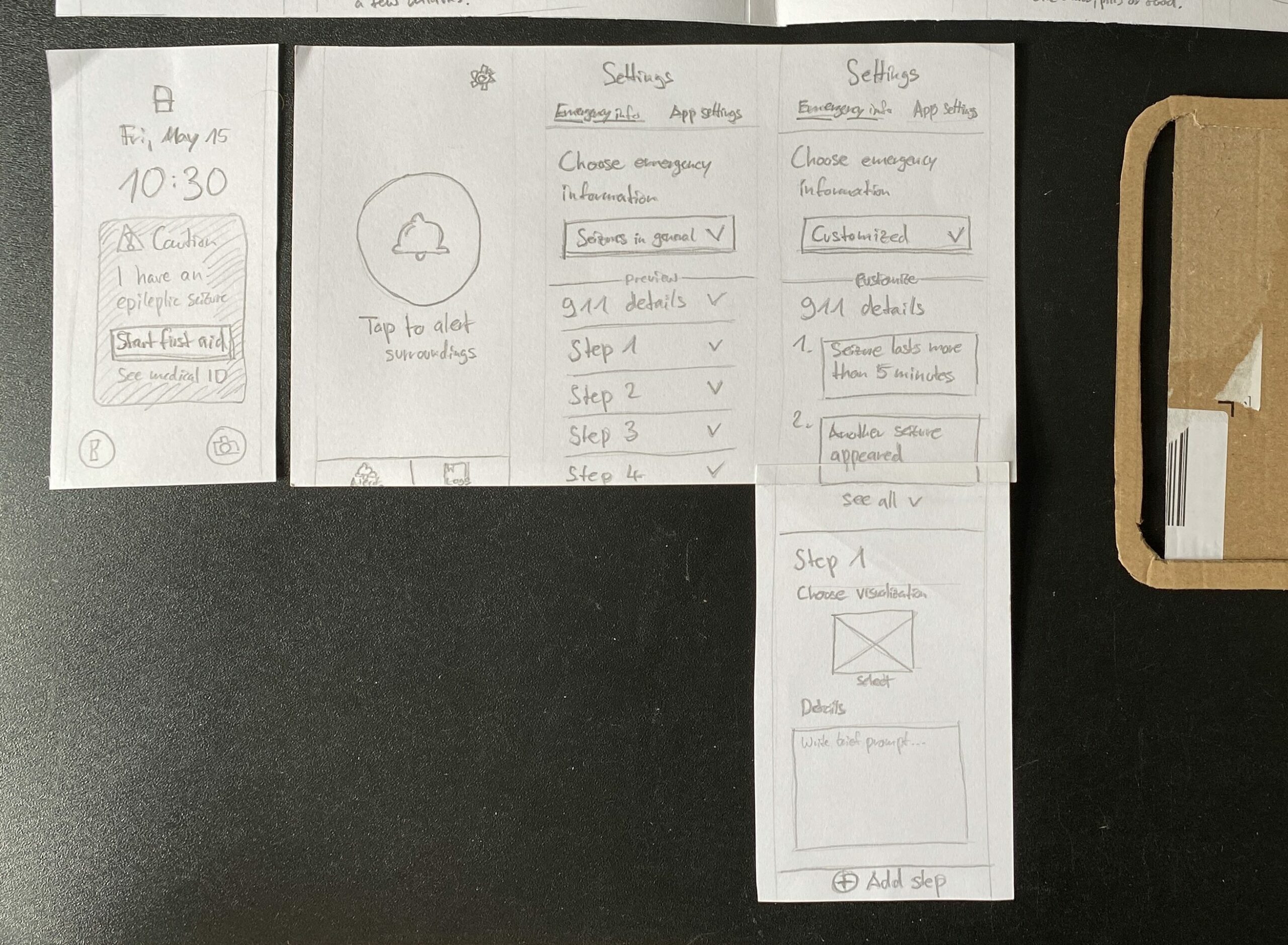
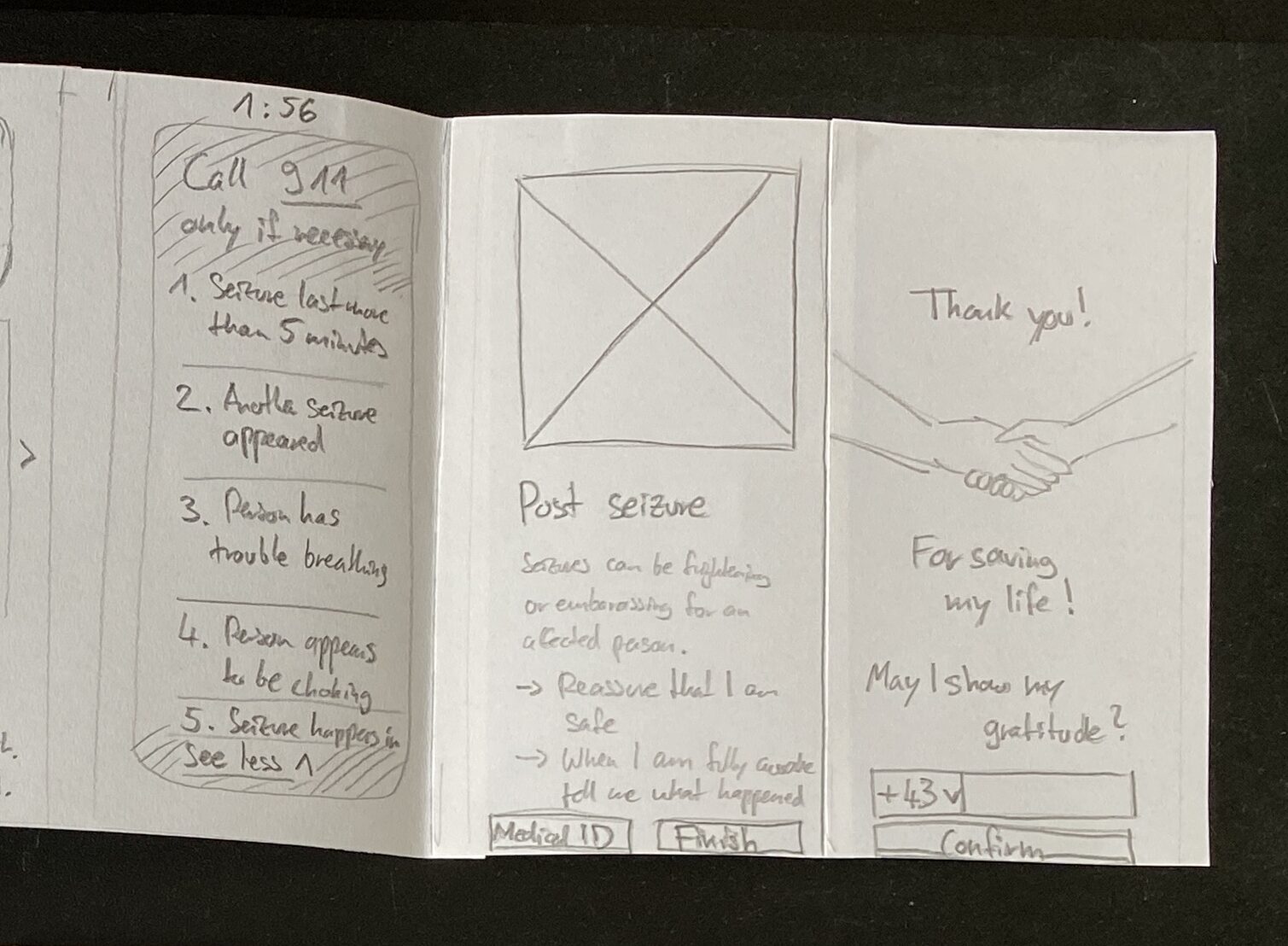
The present prototype represents a mobile app, which has to be manually activated by persons with epilepsy in case of emergency, if they notice an upcoming aura. Surrounding bystanders are then addressed by visual and auditory cues to pay attention to the smartphone.
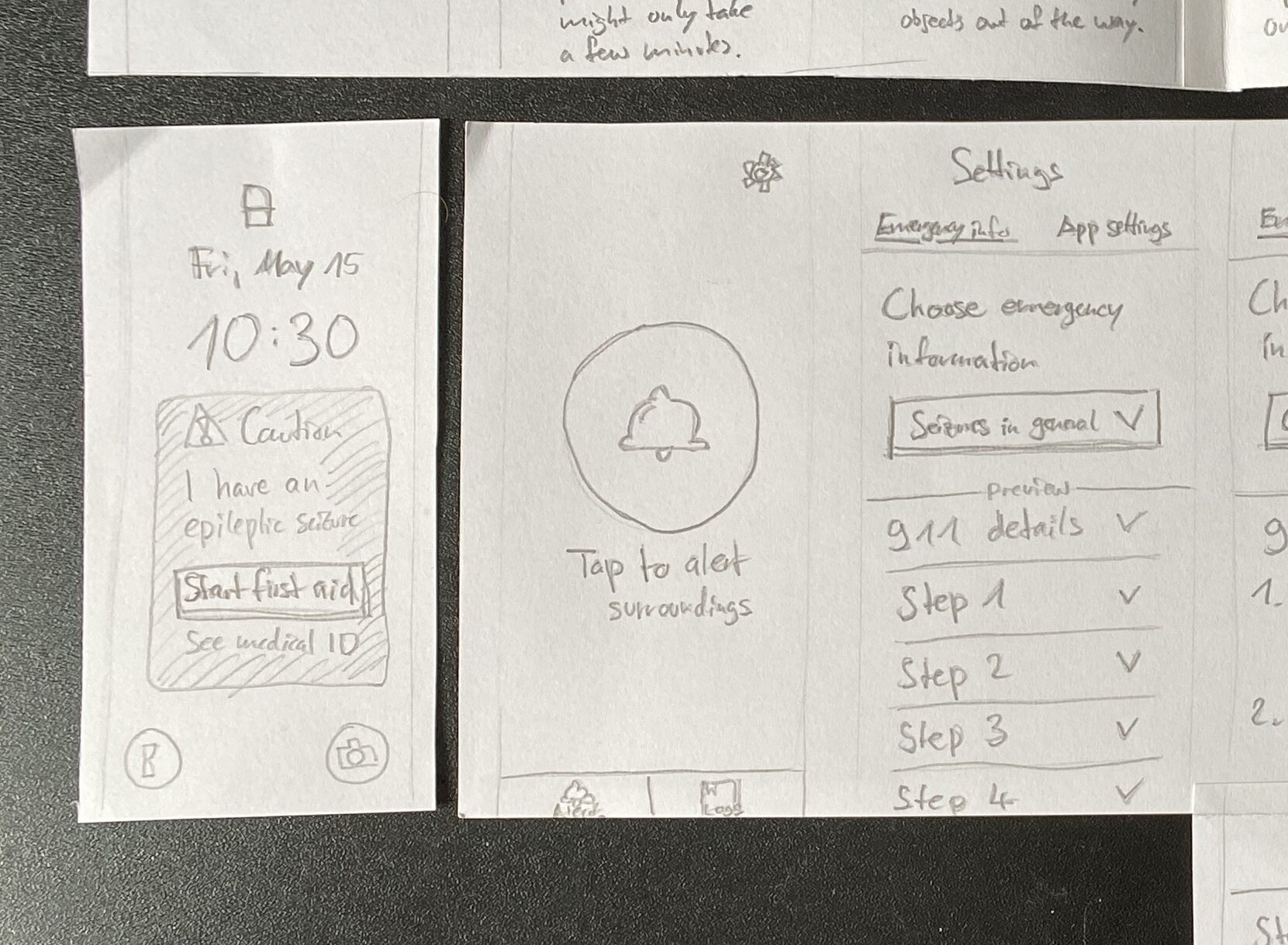
Having a look on the smartphone, bystanders are shown what’s the matter with the person and how to help. This follows a general set of emergency information which is applicable to nearly every type of epileptic seizure. Also bystanders receive information about when it is necessary to call an ambulance.
Advancement: Tailored emergency information
One of the biggest advancements might be the possibility to individually customize emergency information to an affected person’s specific condition. For this I added customizability to the app’s settings. Besides the general emergency information, which is set as a default, users are able specify the shown information steps to their own needs. A visual representation (picture, pre-made illustration etc.) and a short textual instruction in a few sentences can be chosen, and further steps can be added.
Advancement: Findability of medical ID
Another addition is a lock screen widget, once an alert has been activated by the person with epilepsy. In case of a locked phone, this piece helps to give an understanding and access to the first aid instructions as well as the medical ID. The latter is a often hidden feature on mobile operating systems, which gets more visible with the widget once an alert has been started.
Advancement: Expressing gratitude to bystanders
Lastly another advancement could be an extended way to end the app experience, when a seizure has been overcome: Besides communicating appreciation and recognition for the provided help, bystanders can optionally leave their contact details (e.g. a mobile number) for the affected person. Afterwards the rescued person is able to get in touch with its helper.
Auditory cues
As recommended by experts mentioned in the previous blog post the auditory level should play an important role as well, when it comes to the smartphone’s findability and support to follow first aid instructions. Obviously a paper prototype can not provide sound due to its material. This is where a, at least partly, digital component have to come in.
Next steps
Iterating and extending the paper prototype was quiet easy and quick. However its detail has to undergo refinements and the eventualities for various circumstances have to be considered. At this point it makes sense to transfer this haptic paper prototype into a digital prototype, to be able to add interactivity and sound.
As stated in blog post #11, the previous thoughts on my research journey were accompanied by doubts about the relevance and ability to make a serious contribution to the current state of research. To overcome these doubts, I allowed myself to dig deeper into the application areas mentioned that I could possibly focus on:
Ad Hoc First Aid Care Collaboration with the Public
Semi-Ad Hoc Care Collaboration During Transportation
Prior Education for Secondary Caregivers at Workplace/School
The „Ad Hoc First Aid Care Collaboration with the Public“ approach still interests me the most and is the area that is most in demand according to the experts1. This is why I started here.
Ad Hoc First Aid Care
In my research last semester, I realized that there are very few solutions when it comes to mobile applications and wearable technology. Some seem to be poorly designed, others are still in the concept stage, or seem to be no longer in operation. I looked at the following solutions in particular:
Seizure First Aide by the Epilepsy Foundation Minnesota2
Aura: Seizure First Aid by PT. Supremasi Astadaya Sentosa4
Medistat Seizure SOS by Saksham Innovations Private Limited5
For the evaluation, I made a comparison of how these solutions matched the results of my previous research. Early on, I realized that the only serious candidate I could consider, according to my findings and the experts‘ recommendations, was Aura: Seizure First Aid. By coincidence, the designers had the same idea for the app as I did and were inspired by the same content provided by the Epilepsy Foundation.6
Evaluation of Aura: Seizure First Aid
Aura: Seizure First Aid’s core features include the following:
This application addresses the following findings and recommendations as follows:
Conclusion
All in all, Aura: Seizure First Aid already meets the majority of my findings. The app is reduced to providing a general step-by-step approach to securing a person with epilepsy with a great user experience. The affected person has to start an alarm by simply tapping on the app. Their smartphone will then alert nearby bystanders to help and make a decision if an ambulance is needed. As soon as the seizure is over, the process ends with thanking the first responders for their help.
Because epilepsy comes in many different forms, it is highly individualized for each person. Participants in the study expressed a desire to provide bystanders with individually relevant information. Therefore, a mobile app could also allow users to customize the information displayed.
In addition, the general public rarely knows where to look for medical information about a person experiencing a seizure. Therefore, making the information more visible and accessible could be another addition. This could start on the lock screen of the phone.
Stories from people with epilepsy reveal a desire to thank bystanders after they have helped. Sometimes this is not possible because the person has not regained consciousness yet. Providing an extended way to contact helpers after a seizure could be another meaningful contribution.
Next steps
Taking into account my findings, the given app can be extended to meet the needs of a similar target group that values customizability when it comes to shared emergency information. This could be an approach where I can start working on a paper prototype.
Resources
Aehong Min, Wendy Miller, Luis M. Rocha, Katy Börner, Rion Brattig Correia, and Patrick C. Shih. 2021. Just In Time: Challenges and Opportunities of First Aid Care Information Sharing for Supporting Epileptic Seizure Response. Proc. ACM Hum.-Comput. Interact. 5, CSCW1, Article 113 (April 2021), 24 pages. https: //doi.org/10.1145/3449187↩︎
In the first semester I was able to get an insight into how epilepsy first aid could be supported by technology. To take things further, I would like to start with a brief reflection on how the findings and recommendations of this research can be further processed for a real-world prototype and what the next steps might be.
Thoughts on research journey
After taking some time to reflect, I began to doubt how my previous research could lead to a meaningful contribution, since this topic is very focused on a specific use case (emergency) for a specific disease pattern (epilepsy), and there seem to be some promising solutions already out there.
To come to a conclusion, I see three options on how to proceed:
Option 1: Continue with my topic and start prototyping ideas. This would mean no more research than usual.
Option 2: Stay close to my previous research, but eventually choose a different use case or project approach. If necessary, look for similar areas where my research knowledge can be applied. In case of a change of direction, this could mean additional research.
Option 3: Completely change the topic. This would mean the highest amount of (new) research needed and could possibly lead to time constraints.
Weighing the options, a path between options 1 and 2 seems to make the most sense: The first step would be to recall my research findings (pain points, recommendations, etc.).
Next, I should try to evaluate how existing solutions align with what I have learned about the pain points of the target audience and the recommendations of the experts (option 1) to see if there is room for improvement or if a custom concept is even needed.
At the same time, I should be open to following other project ideas if the room for a serious contribution is too small or non-existent (option 2).
Given that this research phase is focused on prototyping, it is of course important to gain more insight into users and stakeholders.
Project approaches to follow
During my previous research, I found expert advice on areas of possible projects1. These include:
Ad Hoc First Aid Care Collaboration with the Public
Semi-Ad Hoc Care Collaboration During Transportation
Finding a Person in Charge & Care Information Sharing When Utilizing Public Transportation
Seizure Monitoring & Information Sharing While Driving
Prior Education for Secondary Caregivers at Workplace/School
After a second look at what I’ve found out, I want to start evaluating existing solutions for „Ad Hoc First Aid Collaboration with the Public“, which according to the experts is the area that is most in demand. At the same time, it has my greatest interest.
Resources
Aehong Min, Wendy Miller, Luis M. Rocha, Katy Börner, Rion Brattig Correia, and Patrick C. Shih. 2021. Just In Time: Challenges and Opportunities of First Aid Care Information Sharing for Supporting Epileptic Seizure Response. Proc. ACM Hum.-Comput. Interact. 5, CSCW1, Article 113 (April 2021), 24 pages. https: //doi.org/10.1145/3449187↩︎
Over the past three months, I have primarily conducted literature research on the overall topic of First Aid Assistance for Chronic Diseases. During this process, this topic has evolved in diverging and converging research phases, becoming more and more detailed over time. At this point I would like to briefly recapitulate what I have learned so far.
Research development
With the announcement of my research topic, I got to know better what first aid and the chain of survival means. I also got a great impression of what interactive first aid applications exist and what areas they cover.
In the beginning, I started to keep the topic very rough, which allowed me to discover things. To understand what first aid consists of, I drew a bigger picture of the different aspects. I also had a first idea of what types of chronic diseases could be considered. Very early on, I realized that I was interested in the specific context of sudden emergencies.
As I delved deeper into the variety of chronic diseases, I discovered types that were suitable and less suitable for my research. I also learned the difference between diseases, symptoms and disease events. The candidates were cardiac arrhythmia, diabetes and epilepsy. What makes epilepsy different from the others is that not every seizure is life threatening. I found this interesting. That is why I decided to pursue this path in my research.
I looked deeper into epilepsy first aid and found a general approach that can be applied to any type of epileptic seizure: Get the person into a safe state and recognize when it is time to call an ambulance. So there is a difficult decision-making process involved.
I was lucky enough to find this very valuable scientific article that describes the current state of research for my central research question: How can we use technology to support first aid? This helped me immensely to understand the criteria that need to be considered, the pain points of people with epilepsy and their families, and recommendations for future technologies to address these issues.
In my search for tools and methods as a starting point for project work, I came across this scientific paper explaining and categorizing different design approaches. It highlighted the possibilities and limitations of design in the strict field of healthcare, which helped me to evaluate where to place a potential project.
Finally, I tried to find out more about untrained first responders who have experience helping a person with epilepsy. This turned out to be very difficult, so I tried to make assumptions about their perspective by studying seizure first aid stories. If further research on this is unsuccessful, I would need to gather information using other (empirical) methods.
Outlook
From this point of research, the next steps would include the following:
Gain greater insight for all stakeholders through additional (user research) methods
Further evaluate existing solutions
Consolidate insights, findings and other information into an initial concept
One of the research questions of my work hasn’t received much attention: „What challenges, needs, and expectations do first responders face?“
In order to include the perspective of first responders, I conducted a literature and web search to see if there was already information available. In terms of time spent, the search so far has been quite difficult. It seems that there is very little information about the experience of untrained first responders in the public area.
However, I was able to find seizure first aid stories published by the Epilepsy Society in the UK. As part of National Epilepsy Week in 2019, they are running a campaign called #seizuresavvy. People were asked to share their first aid experiences, both good and bad.
By studying these stories, I tried to draw conclusions about the challenges, needs and expectations of first responders. The people with epilepsy (PWEs) who contributed their experiences were Vicky, Michael, Chloe, Kas, Tim and Tom. Their stories tell how and who took on the role of first responder. I extracted the information for these three aspects and grouped them into the following five categories.
Education, training, awareness
Effective education and training for first responders is critical, as illustrated by several scenarios involving people experiencing seizures. Rapid decision-making and action are essential in critical situations, emphasizing the need for first responders to seek help quickly and make informed decisions.
There is also a clear call for increased public awareness and education about epilepsy to prevent misunderstandings and ensure appropriate responses in emergencies. Basic first aid skills, such as placing people in the recovery position, can have a positive impact on well-being, highlighting the importance of even simple interventions.
However, challenges exist, including potential misconceptions about seizure first aid, such as the common misconception of placing objects in the mouth. The unpredictable and potentially life-threatening nature of seizures, especially in cases of unstable epilepsy, further complicates the role of first responders.
Advocacy for awareness campaigns and education initiatives is essential to address gaps in public perception and understanding of epilepsy. Individuals such as Chloe and Paula advocate for broader societal awareness, support and understanding, emphasizing the need for education among various groups, including teachers and first responders. The lack of awareness of specific epilepsy conditions, such as photosensitive epilepsy, poses challenges for individuals like Chloe and highlights the importance of comprehensive education and resources.
Communication
Effective communication plays a critical role for first responders in emergency situations. In one scenario, a five-year-old niece had to effectively communicate the emergency to get help from neighbors and emergency services, highlighting the importance of clear and concise communication, even in difficult circumstances.
Vicky probably expected her niece to communicate the situation to the emergency services, underscoring the need for effective communication to ensure a rapid response. In a different context, Tim faces the challenge of recognizing the onset of a seizure, particularly during activities such as running, where rapid communication to bystanders and their response is critical.
Tim’s experience also highlights another aspect of communication challenges – the lack of opportunity for acknowledgement. Despite receiving first aid, Tim was unable to express his gratitude and thanks to those who helped him during the incident. From the first responder’s perspective, they must assume that they will not receive conscious recognition from the individual. This underscores the importance of providing opportunities for individuals to recognize and appreciate the help they receive, thereby contributing to a sense of gratitude and recognition within the community.
Structural circumstances
The structural circumstances surrounding first responders highlight crucial aspects of recognition, support, and challenges faced by individuals like Chloe. As a student, Chloe expects recognition of her epilepsy as a legitimate medical condition and anticipates knowledgeable and supportive responses from teachers and first responders during seizures.
However, stigma poses a significant challenge, as Chloe’s primary school teacher doubts the authenticity of her seizures based on her appearance, and secondary school first responders refuse to help because of the perceived violence of seizures. This underscores the importance of addressing misconceptions and promoting understanding to eliminate stigma in educational and healthcare settings.
Establishments such as supermarkets are also implicated in these structural circumstances. There’s an expectation that such places should have policies and procedures in place to support people experiencing seizures, ensure their safety and prevent them from being left alone after an episode.
The findings underscore the critical need for increased education and training for teachers and first responders. This includes recognizing the type of seizure a student, teacher, employee or customer is having and responding appropriately.
Supportive environment
Creating a supportive environment for persons with epilepsy (PWE) involves a combination of knowledge, training, and understanding of different circumstances.
For example, Vicky teaches her niece about seizure response and emphasizes the importance of preparedness.
In Michael’s case, there’s a potential need for emergency response training for his family, especially Paula, given the unpredictable and severe nature of his seizures. This highlights the importance of ongoing education and preparedness for families living with epilepsy.
Chloe needs a supportive environment at school, where teachers and first responders understand her condition and offer help without stigma. This highlights the need for awareness and understanding in schools to create an inclusive atmosphere for persons with epilepsy.
Response time
The importance of response time is a common thread in several scenarios involving first responders. Vicky’s niece faced the challenge of acting quickly in a time-sensitive situation when Vicky was about to have a seizure, highlighting the critical nature of timely responses.
For people like Michael, getting help in a timely manner when he is having a seizure is critical because of the potential severity of his condition. The expectation is that those around him can respond quickly to provide the necessary support.
In another context, a store assistant became a first responder in a public setting and faced the challenge of responding to a medical emergency involving a tonic-clonic seizure. This highlights the need for individuals in public spaces to be prepared for timely responses to such situations.
It also highlights the need for support during the recovery phase, as seen with Kas, who requires assistance in regaining consciousness and ensuring a safe environment following the seizure. This further emphasizes the time sensitivity not only during the seizure itself, but also in providing support in the aftermath.
Conclusion
Overall, finding experiences from untrained first responders in public settings has been difficult. It is easier to find experiences from persons with epilepsy and those around them than from strangers.
It is questionable whether a more in-depth literature and web search would reveal more information. It could be assumed that previous research and resources do not cover the experiences of untrained bystanders if they are not known or it is not important for them to share their perspective. In order to include their perspective, it may be necessary to reach out to them by initiating an open call or something similar.
Referring to the authors‘ suggestions for innovative approaches in the previous blog post, I conducted further divergent research on existing solutions in the following areas:
Ad Hoc First Aid Care Collaboration with the Public
Semi-Ad Hoc Care Collaboration During Transportation
Prior Education for Secondary Caregivers at Workplace/School
Research criteria
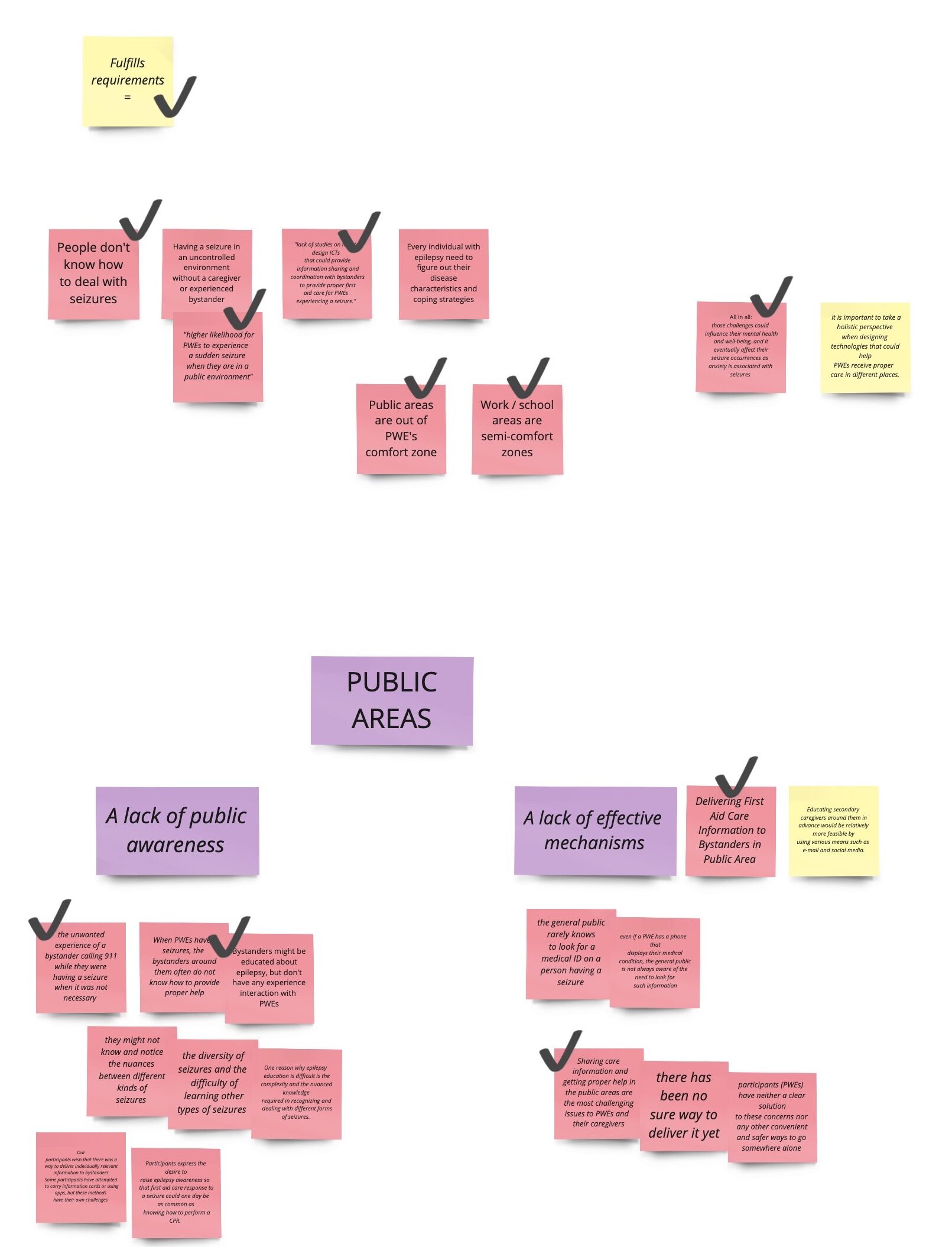
Due to the fact that the authors propose innovative solutions, I noticed a general lack of existing solutions during my research. Looking at the identified pain points that people with epilepsy (PWE) face, I assumed that bystander first aid in public was the most desirable and interesting area. Also, the solutions for this topic are more tangible. I came up with the following criteria to search for:
A solution must work for all types of seizures in general, as they are very individual and the differences are not well known.
A solution must provide information about when to call 911. This is not always the case when a seizure occurs.
A solution must guide untrained bystanders to provide first aid in an emergency, as they may be able to place a person in a safe condition to prevent injury.
A solution must make emergency information clearly visible and accessible to bystanders and medical professionals, otherwise it may be overlooked.
Mixed reality
HoloCPR
Although this solution addresses cardiopulmonary resuscitation (CPR), the authors propose to adapt this concept to epilepsy. HoloCPR is a mixed reality interface that assists bystanders in providing first aid by providing visually augmented user guidance. The developers, associated with UC San Diego – Jacobs School of Engineering and UC San Diego Design Lab, found that this technology can reduce the response time and ease of first aid actions compared to using a tablet application.
Other than this solution, I have not been able to find a virtual reality, augmented reality or mixed reality solution that is specifically tailored to epilepsy. Furthermore, for this concept to work, mixed reality devices need to be further integrated into our daily lives, as seizure emergencies are unpredictable and bystanders need to have the technology with them.
Mobile apps
Aura: Seizure First Aid
Aura is an app designed to help people with epilepsy by alerting their environment and caregivers when a seizure is imminent. Other key features include step-by-step seizure first aid instructions, access to medical IDs, live location sharing, and tracking events in seizure logs.
In doing so, the app provides an all-in-one solution that attempts to cover multiple application areas.
Medistat Seizure SOS
Medistat Seizure SOS takes a similar approach. It is designed to empower epilepsy patients by alerting those around them to seek help: When a seizure occurs, the app notifies nearby bystanders and provides them with audio instructions to effectively provide first aid to the person with epilepsy. Opening the app automatically sends alerts and SMS messages to pre-defined emergency contacts. The app actively and continuously tracks the live location, ensuring that caregivers are constantly updated on the individual’s exact whereabouts.
However, based on app store numbers and reviews, this app appears to be under-utilized.
Wearable devices
MyID
MyID allows you to store your entire medical profile, including emergency contacts, vital signs, medical images, and more. This online profile is linked to a MyID wristband that allows medical professionals and bystanders to access detailed medical information via a QR code.
Compared to traditional medical ID wristbands, where health information is engraved on a small surface, MyID allows users to store an unlimited amount of information in the digital space. However, these devices can be overlooked by untrained bystanders who are the first on the scene in the event of a seizure emergency.
Dialog
Dialog is a concept for an epilepsy aid that focuses on seizure monitoring and detailed reporting. It is a wearable module that can be attached to the skin either by a transparent adhesive or by a watch-like clip. It is also capable of providing early warnings so that a person can prepare to move to a safe state, and a separate bystander app provides step-by-step instructions on how to help a person in an emergency.
This technology concept is beneficial for the end user, who can decide where to wear the module and how visible it is. On the downside, it requires bystanders to install a separate app, which prevents most people in public from acting as first responders.
Conclusion
As I researched existing solutions, I realized how few there were. These examples give a sense of where the industry might be today.
Regarding the Indiana University Bloomington research mentioned in previous blog posts, evaluating existing solutions using the pain points from the research can reveal optimizations.